Individuals consuming more plant-based diets have lower rates of overweight and obesity than those whose diets include or emphasize meat and refined foods.
Abstract
Individuals consuming more plant-based diets have lower rates of overweight and obesity than those whose diets include or emphasize meat and refined foods.1–4 Plant-based patterns are lower in fat and cholesterol and promote both weight loss and long-term healthy weight maintenance.5 Fiber and water in whole plant foods promote satiety with lower caloric density more than animal-based foods, thus allowing the body to reach its natural weight setpoint without deprivation.5, 6
Obesity is a complex disease state involving excessive adipose tissue.7 Overweight and obesity are prominent risk factors for developing metabolic syndrome, heart disease, diabetes, and certain cancers.8 Findings from large-scale epidemiological studies indicate that plant-based diets lead to healthy weight maintenance and reduce both prevalence and incidence of overweight and obesity.1 The American Medical Association designated obesity a disease in 2013.9 As a result, the idea that obesity is caused by insufficient willpower, lack of discipline, and bad personal choices has transformed the public discourse around the condition and reframed it as a disease that increases other health complications and conditions.
Emerging research on the effects of the obesogenic food environment driven by the addictive qualities of refined sugar, salt, and fat, coupled with prevalent sedentary behavior indicates the importance of considering broader environmental conditions when addressing overweight and obesity.10 Plant-based diets help circumnavigate the built environment by normalizing the taste of healthy food and breaking the pull of these addictive ingredients to allow for a healthy weight.11–13
Key Points for Practitioners
- Realistic expectations for any lifestyle intervention is 5–10% weight loss, based on the Diabetes Prevention Program,37 LOOK AHEAD,64 and other trials. There is potential for greater weight loss with a WFPB diet, but more research is needed.
- Many patients are interested in making dietary changes, and a WFPB diet can be offered as a safe and effective option for losing weight and maintaining a healthy weight, independent of increasing exercise.45, 81, 82
- The dietary patterns that seem most advantageous for weight loss and healthy weight maintenance are founded on fruits and vegetables, legumes, and whole grains, moderate or more limited amounts of nuts and seeds, and avoidance of added sugars and oils.1
- Advantages of plant-based diets for weight control include low or no cost of the intervention, as well as reduced risk for metabolic syndrome and other chronic diseases, and improved quality of life.83
- High fiber intake from whole plant foods has been associated with decreased risks of diabetes,84 cancer,85, 86 and heart disease.87
- Some evidence suggests that the majority of individuals are able to eat a WFPB diet and consume appropriate levels of total energy in ad libitum conditions and maintain a healthy weight,45, 50 while a certain minority may need more structured meal plans or portion control to prevent overeating.65, 88 In a recent residential feeding study comparing a low-carbohydrate, ketogenic-style diet (n=11) with a low-fat, WFPB diet (n=10), the WFPB diet led to more significant weight loss, with an average lower ad libitum energy intake of 689 ± 73 kcal d (-1) as compared to the low-carbohydrate diet over 2 weeks (P < 0.0001).89
- Mechanisms through which plant-based diets improve weight outcomes include greater satiety and reduced energy density due to high fiber content, reduced fat, and avoidance of refined foods.90, 49
- Some research suggests that good adherence is the most salient predictor of successful weight loss for overweight patients, over and above any particular diet. While this may be true in theory, WFPB diets pose some particular advantages for those susceptible to food addiction in that for some individuals, it may be easier to avoid refined foods entirely than to cut back on them.65, 91
- Existing evidence on plant-based diets and healthy weight can be communicated to patients to support their ability in order to make informed decisions about their diet and course of treatment.
- If patients express interest in trying a WFPB diet of some kind, it is helpful to share educational and support resources with them.
Obesity in Context
The Obesity Medicine Association defines obesity as a chronic, progressive, relapsing, and treatable multi-factorial neurobehavioral disease wherein increased body fat promotes adipose tissue dysfunction and abnormal fat-mass physical forces, resulting in adverse metabolic, biomechanical, and psychosocial health consequences. Obesity and overweight are defined with cutoffs for body mass index (BMI = kg/m2), the standard calculation to estimate adipose tissue, which is also frequently used to predict chronic disease risk.7, 14
Obesity is often divided into subcategories:
- Class 1: BMI of 30 to < 35
- Class 2: BMI of 35 to < 40
- Class 3: BMI of 40 or higher
Individuals with a BMI of >25 and < 30 are categorized as having overweight, while those >30 are categorized as having obesity. Class 3 obesity is sometimes categorized as “extreme” or “severe” obesity.
Some organizations, including the Obesity Medicine Association, clarify the specific percent body mass cutoffs of >30% for men and >35% for women, which can be obtained by another measurement used for body composition, the bioelectrical impedance analysis (BIA). It measures body fat in relation to lean body mass and is said to be more accurate than BMI.15 There are various BIA machines available that are more accessible than the Dual-Energy X-ray Absorptiometry scan (DEXA), which is considered the gold standard for clinically measuring body composition. DEXA may not be accessible to many patients due to cost and lack of insurance coverage.
While BMI is relevant for a majority of the population, several key limitations also exist. BMI cannot account for differences in body mass between adipose tissue, muscle mass, bone density, overall body composition, or racial and sex differences, particularly relating to those within the intermediate BMI ranges who hold abdominal fat (central obesity). Thus, it may be an inaccurate disease risk marker for certain groups depending on activity level and body composition.16
Other methods of measuring excess adiposity include measuring visceral fat by DEXA, as well as calculating the body fat percentage via body composition, which is particularly useful for those of Asian heritage and other populations with high levels of diabetes. Though we do not have disaggregated data for many subpopulations whose diet has only recently been Westernized, including Asian Americans, there are some data on waist circumference cutoffs for Asians. An important note for Asians: BMI waist circumference obesity cut points are lower ( ≥ 90 cm for Chinese males compared to ≥ 94 cm for Caucasian males).17
It is useful to consider waist circumference in addition to BMI when diagnosing overweight/obesity,18, 19 as the BMI may mislabel many in certain subpopulations, including older women, the elderly, children, or those with significant muscle mass.13, 16, 20, 21 These limitations notwithstanding, BMI still has substantial utility for assessing cardiometabolic health for a majority of the population.22
Over a billion people around the world are considered overweight or obese. According to the World Health Organization and the Centers for Disease Control, obesity rates have nearly tripled worldwide since 1975, with more than 1.9 billion overweight adults (18 years and older). Of these, over 650 million were obese.12 Though Americans are living longer, they are living with chronic health conditions.23 Globally, 39% of adults aged 18 years and over were overweight in 2016, and 13% were obese. In the US, 2017–18 data shows the age-adjusted prevalence of obesity in adults was 42.4%, with no significant differences between men and women among all adults or by age group.24
Rates of overweight/obesity are more prevalent among some groups than the general population. Non-Hispanic Black adults had the highest age-adjusted prevalence (49.6%), followed by Hispanic adults (44.8%), non-Hispanic White adults (42.2%), and non-Hispanic Asian adults (17.4%).25 The prevalence of obesity was 40.0% among adults aged 20 to 39 years, 44.8% among adults aged 40 to 59 years, and 42.8% among adults aged 60 and older.26 Minority groups are especially challenged as social determinants of health, structural racism, and systemic inequities implicate their ability to engage in healthy eating patterns and physical activity.27–31
Access to refined and fast food as well as disparities in access to healthy foods have contributed to a dietary pattern of excess calories, high levels of animal fat and protein, and refined carbohydrates, which have contributed to the increased rates of overweight, obesity, and negative downstream health consequences.32 Obesity is a core condition for developing metabolic syndrome, the cluster of conditions that increase heart disease risk (increased blood pressure, blood sugar, cholesterol, triglyceride levels, and excess abdominal body fat).33
Both obesity and diabetes have been shown to increase risk for infections and mortality by altering pulmonary mechanics, increasing aggravation of the inflammatory storm, and abnormalities in lung physiology and micrangium, all of which may increase virus infectivity and virulence.34 Both obesity and viruses such as COVID-19 impact lower-income populations and people of color disproportionately, as access to adequate healthcare and nutrition are often lacking due to long-standing inequity embedded in our society.28 Black, Latinx, and Native Americans die of COVID-19 at rates of more than 2.7 times white Americans. The rise in obesity rates since the year 200035 has made obesity an increasingly urgent problem, and sustainable and acceptable dietary solutions are a top priority for healthcare.
Obesity treatment is multi-modal and, depending on BMI cutoffs, may include medication and surgery, endoscopic procedures, and very low-calorie diets. Lifestyle medicine and behavioral therapy are the foundation of obesity treatment. The United States Preventive Services Task Force recommends intensive, multicomponent behavioral intervention for all individuals with obesity.36 These programs include at least 12 sessions in the first year, weekly or even twice per week.36 Many are modeled after the Diabetes Prevention Program (DPP).37 It is important to understand all options available to treat obesity because simply telling a patient they have obesity and must lose weight has been shown to be ineffective for weight loss.38 In fact, telling a patient they need to lose weight without providing adequate treatment can increase obesity stigma, which has been shown to worsen weight loss outcomes. Clinicians should be aware of their own obesity stigma and/or bias, and this implicit or explicit bias should not prevent them from providing all the available options for obesity treatment, including medications and surgery should they be indicated. In addition, being aware of weight bias may help prevent clinicians from exacerbating obesity stigma for patients struggling with obesity.39–42 Obesity treatment should include a behavioral element. In addition to addressing weight bias, behavioral treatment includes a variety of components including collaborative goal setting, problem-solving, planning, stimulus control, social support, addressing emotional eating, self-monitoring, cognitive restructuring, motivational interviewing, relapse prevention, and contingency planning.43
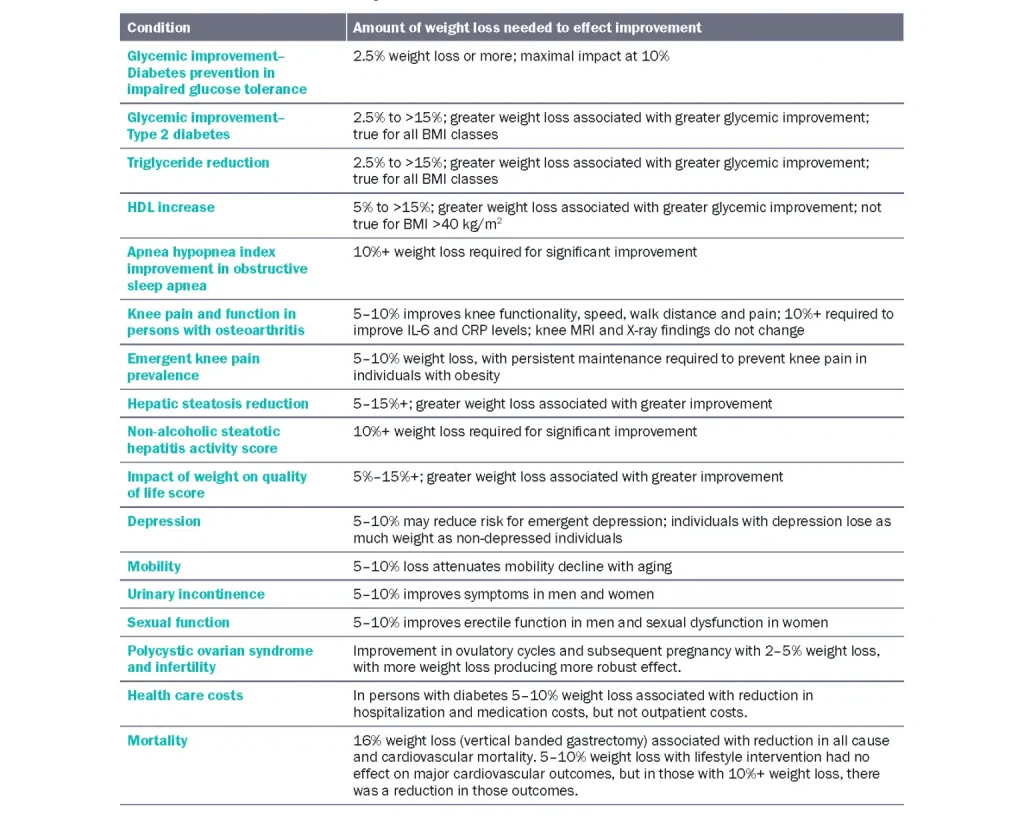 Table 1 Relationship with amount of weight loss and various conditions
Table 1 Relationship with amount of weight loss and various conditions
Ketogenic Diets
Obesity is a chronic, relapsing, and progressive disease.9, 77 Ketogenic diets have been shown to aid in short-term weight loss.78 Since many cultural, social, ecological, and environmental factors influence diet, it is essential to individualize a diet plan for each patient with obesity to maximize adherence,74 and some patients may choose a ketogenic diet. However, the POUNDS LOST study showed that adherence could be more important than diet composition, and if a patient’s preferences steer them towards a ketogenic diet, this may be an improvement compared to their previous diet. Like any treatment plan, ketogenic diets have risks and benefits. Some of the risks include increased mood changes and fatigue, particularly with exercise. There is ample evidence that plant-based diets can achieve equal or superior weight loss to other diets that exclude whole grains, legumes, and starchy vegetables.58 Findings from the ARIC (Atherosclerosis Risk in Communities) study suggest that while mortality risk appears lowest at 50-55% carbohydrate intake, substituting carbohydrates with plant-based protein lowered mortality, while substituting carbohydrates with animal-based protein increased mortality.79 Thus, patients on low carbohydrate diets should be encouraged to maximize their fruit and vegetable intake.
Given concerns about cardiovascular risk, patients with coronary artery disease or history of myocardial infarction who decide on ketogenic diets should be advised of these risks, and cholesterol levels should be monitored carefully. Additionally, patients on ketogenic diets should be monitored for bowel symptoms and abdominal discomfort as they are at risk for decreased intake of soluble and insoluble fiber as well as resistant starch and fructooligosaccharides. The long-term effect of the ketogenic diet on the gut microbiota is yet unclear. Physicians supervising patients on a ketogenic diet should consider supplementation with inulin, lactulose, fructooligosaccharide, and galactooligosaccharides to increase the population of Bifidobacterium.80
Mechanisms
Plant-based diets have consistently been associated with reduced body weight because they directly address the primary dietary mechanisms that lead to reduced body fat.92 The mechanisms by which WFPB diets support healthy weight maintenance and weight loss include reduced energy density, increased satiety, avoidance of addictive foods, and positive benefits for the gut microbiota. With obesity, adipose tissue and visceral fat expansion cause compression, joint stress, metabolic disorders, organ dysfunction, and increased mortality.93 The increase in peripheral and central fat mass is a chronic and potentially reversible process. Conversely, the expansion of adipose tissues and visceral fat leads to organ dysfunction and an increased risk of mortality. Such an increased risk of mortality and morbidity can also affect metabolically healthy individuals with obesity with disease progression.13
Energy Density
The mechanisms by which plant-based diets cause weight loss hinge on reduced dietary energy density due to their higher fiber, higher water, lowfat content, and increased postprandial energy expenditure.94, 95 Energy density is the amount of energy in a particular weight of food, in the form of calories per gram, spanning from 0 to 9 kcal/g, along with its water content. Fat is around 9 kcal/g, carbohydrate and protein are both around 4 kcal/g, and alcohol is 7 kcal/g.90 Foods high in calorie density have a large number of calories per unit weight of food, and foods low in calorie density have far fewer calories per unit weight of food.96 Foods low in calorie density with higher fiber content effectively increase satiety, as volume and fiber content activate receptors in the stomach that respond to being physically full of food.97, 98 Thus, eating high-fiber foods (unrefined, plant foods) makes it possible to fill up on fewer calories without experiencing hunger.96 Foods lower in calorie density include whole fruits, colorful vegetables, starchy vegetables, intact whole grains, and legumes. These are also the foods highest in nutrient density. Therefore, by following a diet lower in calorie density, one also consumes a diet highest in nutrient density. In contrast, animal foods and refined foods are energy-dense, making it easier to overconsume calories without a need. Table 2 presents a sample of energy and fiber content of select plant, animal, and highly processed foods, demonstrating that, overall, unrefined plant foods maximize fiber consumption and allow one to eat food with lower energy density.
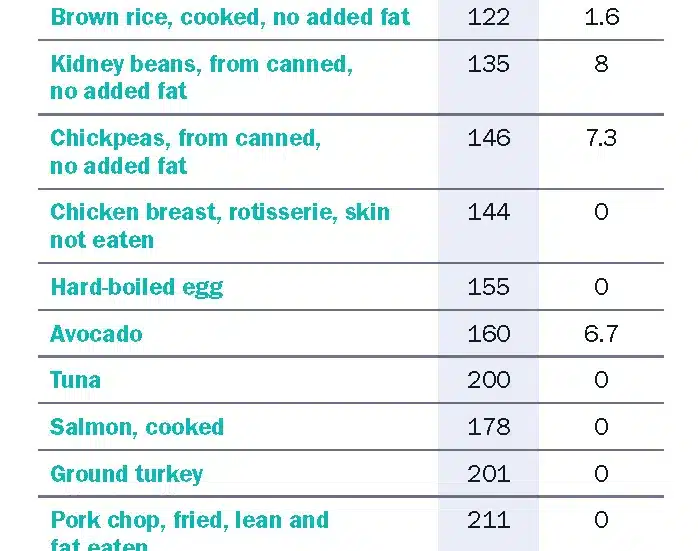 Table 2 Energy and fiber content of a selection of plant, animal, and highly processed foods (per 100 grams)99
Table 2 Energy and fiber content of a selection of plant, animal, and highly processed foods (per 100 grams)99
Fiber
Fiber is found only in plant foods99 and is an essential component of a healthy eating pattern, as high fiber consumption is associated with overall lower chronic disease. Higher fiber consumption is a hallmark of plant-based diets,100 and in observational studies, individuals consuming omnivorous diets frequently do not meet fiber recommendations while those consuming increasingly plant-based diets do.101, 102 Higher fiber intakes increase satiety, a key component of reduced energy consumption, and higher fiber consumption is implicated in weight loss.103 Highly processed foods lacking intact fiber make up the bulk of calories consumed in America,104 facilitating overconsumption and weight gain. These foods have become progressively cheaper and easier to access in the modern food environment.104
Gut Microbiota
Microbiome dysbiosis that promotes bile acid fermentation is associated with obesity.92 Mechanisms may include impeding the abundance and variety of intestinal flora from excessive intake of unhealthy foods and lack of dietary fiber. The fermentation of fiber appears to be a factor in a host of mechanisms related to obesity, including intestinal barrier function, glucose function, and appetite regulation.105 Short-chain fatty acids (SCFAs) produced by the gut microbiota through its digestion and fermentation process can modulate satiety and eating patterns, and regulate energy intake through appetite. SCFAs can also suppress intestinal mobility transit and allow for a higher uptake of nutrients.106
Whole Plant Foods’ Effect on Satiety
Whole food, predominantly plant-based diets, have a number of characteristics that increase satiety, a key element of weight loss. Whole plant foods increase satiety more than highly processed foods lacking intact fiber to hold water and macronutrients in the stomach. Further, solid foods have a greater effect than liquid.107 Water in food is chemically different from water taken as a beverage as it leaves the stomach more slowly and improves satiety.108 The fiber in unrefined carbohydrates enhances satiety without adding calories. Fiber-filled foods require greater mastication, which reduces the ingestion rate, increases stomach distention, and promotes satiation. Soluble fibers delay gastric emptying and may be linked to the “second meal effect, delaying the return of hunger.109 Though protein has demonstrated a higher satiety effect than carbohydrate, trials usually compare a ketogenic-style diet to a conventional American Heart Association diet of 30% fat (which is not very low-fat) to a diet that includes refined and processed low-fat animal foods; whole food diets are not typically included.
Food Addiction and Hyperpalatable Foods
Both food and drug dependency activate similar neural circuitry inducing biochemical change in the brain that can lead to craving beyond need.110,111 Highly processed foods made of concentrated fat, sugar, and sodium are created to surpass the rewarding properties of whole foods such as fruits and vegetables. They cause the release of neurotransmitters dopamine and opioids expressed throughout the limbic system that can reinforce the eating behaviors driving obesity.51 Addictive patterns of excessive eating are often attributed to the stimulating properties of these hyperpalatable foods prevalent in our modern food environment. Food addiction research indicates that it may be preferable for some people to avoid certain trigger foods altogether as opposed to eating less of them.112 A WFPB diet may effectively overcome addiction to hyperpalatable foods in individuals with obesity through the avoidance of trigger foods containing added fat, sugar, and salt.
Significant Weight Loss Using a Plant-Based Diet
In 2021, a critical study comparing weight loss between diets demonstrated the unique benefit for overweight individuals of a minimally processed, plant-based, low-fat diet consumed in ad libitum conditions.89 Those consuming the low-fat, plant-based diet reduced energy intake by approximately 689 kcal/day, compared to a minimally processed, animal-based, ketogenic, low-carbohydrate diet.89 Participants on the minimally processed, animal-based diet lost weight and body fat but reported no significant differences in hunger, fullness, satisfaction, or pleasantness of meals.89
The 2017 BROAD study found that a WFPB diet resulted in similar weight loss at 12 months compared to other diets such as low-carbohydrate and low-fat diet, which led to significant BMI and cholesterol improvements and improvements to other risk factors.5 Similar studies have observed similar weight loss, which is: at six months 12.0 kg reduction (95% CI±1.8), and at one year 10.9 kg (95% CI±1.2) and 12.2 kg reductions (95% CI±1.3); (this last study included telemonitoring113).5 Further, those on the diet had the advantage of eating to satiation without food restriction. In contrast, studies on the effects of low-carbohydrate diets have shown higher rates of all-cause mortality,114 decreased peripheral flow-mediated dilation,115 worsening of coronary artery disease,116 and increased constipation rates, headache, halitosis, muscle cramps, general weakness, and rash.117 Thus, while some evidence exists that low-carbohydrate diets may aid in weight loss, the cardiometabolic side effects are cause for concern, and dietary treatment decisions should be made on an individual basis weighing risks and benefits for the patient, as well as adherence.
Common Questions and Concerns
Don’t carbs make people gain weight?
Though refined carbohydrate products like baked goods are associated with weight gain, increased carbohydrate and fiber intake as part of a plant-based, high-carbohydrate, low-fat diet are associated with beneficial effects on weight, body composition, and insulin resistance.103 WFPB diet is primarily composed of complex and unrefined carbohydrates.100 The healthiest cultures in the world eat a high-carbohydrate diet.118 Carbohydrate quality is important, and complex and unrefined carbohydrates from legumes, vegetables, whole grains, and fruits differ in their health effects from refined carbohydrates found in soda, pastries, cookies, and white bread.119
Doesn’t a low-carbohydrate diet work for weight loss?
Low-carbohydrate diets have produced weight loss in experimental and real-world settings, but the effectiveness is based on energy restriction, not the quality of the diet. Low-carbohydrate diets are typically based on high amounts of animal foods, substituting carbohydrate, the body’s preferred energy source, for fat and protein. The body breaks down protein first and then fat for energy. Low-carbohydrate diets increase LDL cholesterol, which can have long-term cardiovascular effects.89, 120 Substantial reduction of dietary carbohydrate can induce a state of ketosis, which may suppress appetite.
Researchers examining data from The New DIETs study found that non-compliant vegan and vegetarian participants (n=16) were still consuming a more plant-food diet at six months than other groups such as non-adherent pesco-vegetarian/semi-vegetarian (n = 15, −2.3 ± 200.3 mg; P = 0.02) and omnivorous participants (n = 7, 17.0 ± 36.0 mg; P = 0.04).2, 65 Clinicians treating patients on low-carbohydrate diets, such as ketogenic-style diets, should be vigilant in encouraging them to consume healthy whole carbohydrate foods, such as an abundance of non-starchy vegetables, berries and citrus, and those vegetables low in starch but high in resistant starch such as jicama. Some individuals on ketogenic diets have been shown to have reduced exercise tolerance due to higher levels of blood ketones.121 Further, the long-term effects of the ketogenic diet on the gut microbiota are yet unclear. Physicians supervising patients on a ketogenic diet should consider supplementation with inulin, lactulose, fructooligosaccharides, and galacto-oligosaccharides, to increase the population of Bifidobacterium.80
Some research demonstrates greater weight loss among obese subjects on a low-carbohydrate diet compared to a low-fat, plant-based diet, though greater improvements in triglyceride levels and insulin sensitivity have been demonstrated using a low-fat diet of any kind. In a patient-centered decision-making discussion, the physician should weigh the risks and benefits of carbohydrate-restricted diets with the patient, explaining that the ketogenic mechanism ends as soon as individuals stop the diet, often resulting in regaining of weight.122 As with any treatment to overcome disease and decrease mortality risk, including bariatric surgery with its risk of ulcers or dumping syndrome, the benefits in any particular situation may outweigh the risks. The risk of relapse with low-carbohydrate diets is the same as with any other diet.
Some people report they have tried a vegetarian diet in that past and felt hungry.
A vegan or vegetarian diet consisting of processed foods and refined grains may not supply enough nutrients, intact fiber, and water to feel satiated. Legumes and whole grains, potatoes, and soybean products like tempeh and tofu may have been lacking, and these foods allow for the feeling of fullness and satiation.123 Potentially addictive foods with saturated fats and refined sugars may make individuals consuming a vegetarian diet that is not a WFPB diet more hungry. A well-planned, plant-based diet has all the nutrients needed for health (except for possibly vitamins B12 and D), including vitamins A, D, E, C, folate, calcium, magnesium, potassium, and fiber.124 For most individuals, it takes time for the body to get used to the different macronutrient content (a week or two), particularly if one is used to high-density foods such as cheese and meat. Additionally, when eating a less energy-dense diet, it may be necessary to increase food volume to consume enough calories.
Isn’t weight gain a normal part of aging?
Over the lifespan, metabolism naturally slows down, and body composition gradually shifts—the proportion of muscle decreases, and fat increases. This shift makes it easier to gain weight if calorie intake and activity level stay the same. In addition, some people become less physically active as they age, increasing the risk of weight gain.125 For those who continue eating a rich Western diet, weight gain may seem inevitable, but weight gain can be prevented using a high-fiber, plant-based diet and daily physical activity.
No diet has ever worked for me.
Generally, dieting is not associated with long term weight loss. Individuals are challenged by interactions between biology, behavior, and the obesogenic environment.57 A dietary plan often leads to feelings of deprivation and restriction, which is hard to maintain. Losing weight using a nutritive plant-based approach as opposed to a calorically restrictive method may allow for long term success, healthier outcomes, and a healthier relationship with food. Further, food deprivation can lead to hormonal imbalances making us more prone to depression, a common state among dieters. Irritability, anger, anxiety, mood swings etc., are typical for dieters. A low-carbohydrate, high protein diet; low-protein, high-carbohydrate diet; and an energy-restricted low-carbohydrate diet have all demonstrated the effect of synthesis and metabolism of tryptophan, serotonin, noradrenaline, and dopamine.126, 127 Further, when the body senses calorie restriction, metabolism will slow down to preserve energy and burn fewer calories.81, 127 A nutritious, fiber-filled dietary pattern can avoid these pitfalls, as fiber fills the stomach and offers satiety.
I just can’t lose weight from diets.
Though some medical conditions can drive weight gain and prevent weight loss, including hypothyroidism, polycystic ovarian syndrome, and sleep apnea, for most individuals, weight is determined by energy intake vs. energy expenditures (calories in vs. calories out). Energy balance, the relationship between intake and expenditure, is affected by various dietary factors and physical activity behaviors. In the obesogenic modern food environment, it is extremely easy, for reasons previously discussed, to consume more energy than needed. According to a 2014 study, about 19.9% of people in North America and Europe satisfy the criteria for food addiction.128 Further, weight loss can be a slow process, and many people have unrealistic expectations. Research indicates that any diet may work with consistent adherence,129 but a nutritious plant-based diet may resolve many of these roadblocks related to satisfaction and enjoyment and become a life-long healthy alternative to unhealthy eating patterns.
Summary of Key Studies
We extracted data on 12 of the strongest studies in our review, all of which examine the role of vegetarian and vegan diets and plant-based food groups on weight loss and healthy weight maintenance (Appendix Table 1). Of the twelve, seven studies were randomized controlled trials or crossover trials,5, 103, 130–134 three were systematic reviews (SR) and meta-analyses (MA),70, 135, 136 one was an MA,137 and one was an observational study on the EPIC cohort.54 Of diets and components studied, six studies examined low-fat, plant-based (LFPB) diets or WFPB diets,5, 89, 103, 130, 131, 133 one examined the effect of total fruit and vegetable consumption on weight gain,54 one examined the effect of dietary substitution of pulses on weight gain,136 three studies examined a mix of vegan, various versions of vegetarian, and omnivorous diets on weight132, 135, 137 and one examined the effect of total plant and animal protein on weight gain.54
Of studies examining LFPB diets, most found significant associations between LFPB diet and weight reduction. Thomson et al. found that the intervention group had significant drops in BMI, LDL cholesterol, and HbA1c, signifying improved glycemic control.131 A study of GEICO employees found that LFPB intervention significantly reduced weight at 22 weeks compared to the control group, with greater adherence correlating with greater weight loss. Wright et al. found significant reductions in weight, reductions in blood lipids, and increases in quality of life, in addition to improved HbA1c compared to controls at 12 months of follow-up.5 Kahleova et al. found that LFPB diet intervention led to significant decreases in fat mass and visceral fat volume, in addition to improved glycemic control.103
One RCT found that the LFPB diet was superior to the Mediterranean diet in eliciting weight loss, reducing homeostatic model assessment of insulin resistance (HOMA-IR), blood pressure, and lipids.133 Another RCT found that an LFPB diet produced reduced energy intake in an ad-libitum setting compared to a low-carbohydrate ketogenic diet. In addition, weight loss on the LFPB diet resulted in fat mass loss, while weight loss on a ketogenic diet resulted primarily in loss of fat-free mass, such as water and muscle.
One study examining food components found significant associations between animal protein and total protein consumption and weight gain but no significant association between plant-protein consumption and yearly weight gain.54 A study examining fruit and vegetable consumption found significant associations between fruit intake and weight reduction, waist circumference, and BMI, and a reduced risk of adiposity in high quantiles of fruit and vegetable consumption compared to the lowest quantiles.70
Another study examining pulse consumption and weight outcomes found that isocaloric substitution of pulses into the diet resulted in small but statistically significant reductions in weight.136
Of studies examining various diets’ effects on weight loss, it was generally found that vegetarian diets resulted in weight loss to a greater extent than other diets. A meta-analysis by Barnard and colleagues found that vegetarian diets resulted in weight loss regardless of whether weight loss was the study’s goal. However, studies in which weight loss was a primary goal found greater reductions in weight than other studies.135
Finally, a random control study by Moore et al. compared weight loss outcomes between vegan, vegetarian, pesco-vegetarian, lacto-ovovegetarian, and omnivorous diets, finding that of nonadherent participants, those randomized to vegan and vegetarian diets experienced a greater reduction in weight than other non-adherent participants. Though, in adherent individuals, there was no mean difference in weight change at follow-up.132
Promising Results—Examples of Disease Reversal
Many people feel demoralized after failing to lose weight and keep it off to control chronic health conditions associated with being overweight. These case reports reflect the relief that many patients experience using a WFPB diet to effectively treat cardiometabolic risk reduction and weight loss. The prescriptive solution to rising obesity prevalence caused by increased convenience and marketing of high-fat, low nutrient food is the use of a high fiber, high carbohydrate dietary protocol, which is both therapeutic and sustainable over the long term. A low-fat, plant-based diet shows the possibility of significant weight loss both in short-term studies, as well as maintaining weight loss over the years.81, 138, 139
54-Year Old Woman Loses 50 Pounds in 6 Months
A 54-year-old female with a grade 3 obesity, BMI of 45.2 kg/m2, and type II diabetes (hemoglobin A1c 8.1%) succeeded in losing 22.7 kg and reversed her diabetes without the use of medications using a WFPB dietary pattern. After suffering from lower extremity edema, her x-Ray revealed lower extremity atherosclerosis. She was started on a beta-blocker, an ACE inhibitor, and a statin. She underwent cardiac catheterization revealing a cardiomyopathy of a 30% proximal left anterior descending artery stenosis, a 25% proximal and a 60% distal left circumflex artery stenosis, and a 65% first obtuse marginal artery lesion.140 Shaken by her diagnosis, she became determined to adopt a healthy WFPB diet. She lost 22.7 kg in <6 months. Her diabetes resolved, with her hemoglobin A1c falling to 5.7% without the use of diabetes medications. Her baseline dyspnea on exertion improved considerably, and a repeat echocardiography in six months revealed a normal left ventricular ejection fraction of 55%.140
50-Pound Weight Loss and Reversal of Comorbidities in 9 Months
A 65-year-old male diabetic veteran lost 50 pounds after surviving two heart attacks within 62 days and triple bypass surgery. After participating in a Veteran’s Hospital-sponsored Heart Disease Reversal Program, he adopted a WFPB diet under the watch of the program’s doctor. He lost 9 pounds in the first month. At three months he was completely free of his angina, and at 9 months lost 50 pounds, and his diabetes medication was cut in half.141
Conclusion
To date, there is a wealth of data from observational and clinical studies establishing improvements in body weight using a healthy, plant-prominent diet, apparently attributable to reduced dietary energy density and increased postprandial energy expenditure. In addition to weight loss, plant-based diets led to favorable changes in overall nutrition, plasma lipid concentrations, blood glucose, and blood pressure, which lowers risk and, in some cases, reversed chronic comorbidities. In summary, the body of evidence presented here suggests that low-fat, plant-based diets and WFPB diets effectively reduce weight, reduce blood pressure, improve glycemic control, and reduce fat mass among individuals with obesity, as well as prevent weight gain.
CONTINUE READING IN THIS SERIES
Download the Full Series
Benefits of Plant-Based Nutrition
Get the full Benefits of Plant-Based Nutrition series in a single PDF — including in-depth footnotes and research references available only in the downloadable version. Perfect for clinicians, educators, or anyone who wants the full science behind the story.
Acknowledgement
This review was made possible in part due to a generous donation from Kate Farms. For more information on Kate Farms please visit their website here. www.katefarms.com