Cancer prevention is too often reduced to screening and early detection, overlooking the daily lifestyle patterns and upstream conditions that shape risk long before disease appears.
It’s a routine visit. A patient sits across from their primary care clinician, relief softening their shoulders as they hear, “Everything looks good.” They step back out into their day, phone already buzzing with reminders. Lunch is a package from the break room vending machine, eaten quickly beneath fluorescent lights.
That familiar ache in their neck returns as they hurry back to their desk, another afternoon without sunlight. They had left their appointment reassured, but nothing has changed about the long sedentary hours, the habits of grabbing food on the go, the chronic stress, or the interrupted sleep shaped by their environment.
No disease has been detected, but the conditions that shape risk remain untouched. This is where prevention lives — not in a single appointment, but in the patterns that unfold between visits.
Detection is not prevention
Population studies show that while cancer screening is widely recognized, awareness of lifestyle factors that influence cancer risk remains uneven, particularly across socioeconomic groups.
For example, adults with higher incomes are more likely to be aware that diet and activity affect cancer risk compared to those living below the poverty line, highlighting how prevention is commonly framed around detection rather than risk reduction.
For both individuals and clinicians, cancer prevention is frequently reduced to screening — scheduling a mammogram, a colonoscopy, or routine blood work. These tools are essential and lifesaving. But detection is not the same as prevention.
True prevention — in the form of risk reduction — begins much earlier. It unfolds in the environments people live in, the opportunities available to them, and the daily lifestyle patterns that shape their health.
Time constraints, competing priorities, and uncertainty about roles often influence whether lifestyle conversations happen in clinical care. Who should raise the topic? Who is responsible for knowing the recommendations? Do clinicians feel trained — or empowered — to address them? Like many areas of life, when we feel uncertain, we tend to avoid the conversation.
While we cannot eliminate cancer risk entirely — genetics, environment, and biology all matter — we can influence the context in which risk develops. Not only through individual behaviors, but through the systems and environments that shape those behaviors.
Prevention starts upstream
When we talk about prevention, it’s tempting to focus only on individual advice: eat better, move more, reduce stress. But cancer risk is not determined solely by willpower. It is formed by access.
Picture a single parent who faces a familiar decision: pick up a second shift to cover rent or take unpaid time off to bring their child to a checkup. Or someone weighing the cost of a bus fare to the grocery store against settling for processed food at the corner shop. These choices reveal how access shapes the daily realities behind statistics, turning prevention into a privilege rather than a routine.
Across the United States, cancer outcomes increasingly reflect these upstream realities. Lower-income and rural communities continue to experience higher mortality rates and slower improvements in outcomes than urban populations. Differences in transportation, specialist availability, screening infrastructure, and food access all influence who benefits from advances in prevention and care.
When prevention strategies assume equal access, they risk widening disparities rather than reducing them. Effective cancer prevention must therefore address not only knowledge, but opportunity.
Lifestyle medicine makes prevention actionable
Lifestyle medicine provides a framework for translating prevention in daily life. It recognizes that health is built through interacting patterns: nutrition, movement, sleep, stress, connection, and avoidance of risky substances. Together, these patterns influence biological pathways tied to cancer risk.
For example, chronic inflammation is a pathway linking lifestyle habits to cancer development. Persistent inflammation, often driven by poor diet, inactivity, or ongoing stress, can trigger cellular changes that make cancer more likely to arise. Highlighting this connection helps show how everyday choices directly impact cancer biology.
These behaviors do not exist in isolation. Policies, community design, workplace culture, and healthcare systems shape them. Supporting prevention means forming spaces where healthy patterns are feasible, affordable, and culturally relevant. The American College of Lifestyle Medicine’s Lifestyle Medicine Toolkit for Cancer Risk Reduction and Survivorship is an accessible resource that reflects this approach, delivering practical resources that help clinicians integrate prevention conversations into routine care and connect patients with realistic strategies.
For example, a clinician might try asking, “Would you like to talk about one lifestyle tweak that could fit your week?” Simple phrases like this lower the barrier to opening a meaningful discussion, making prevention more approachable for both clinicians and patients.When prevention becomes embedded in clinical dialogue, community design, and policy decisions, it shifts from abstract advice to shared responsibility.
If prevention isn’t just screening, what is it?
The American Institute for Cancer Research emphasizes that cancer risk is influenced not by a single food or behavior, but by overall lifestyle patterns sustained over time. In practical terms, prevention looks like creating a daily environment that supports metabolic health, body composition, and emotional well-being.
This includes:
- building meals around plant foods
- prioritizing fiber and whole foods
- limiting red and processed meats
- reducing ultra-processed foods and sugary drinks
- maintaining regular physical activity
- limiting or avoiding alcohol
These are not rigid rules. Each habit contributes to the whole person. Prevention is not built through perfection, but through repetition of small behaviors over time.
What does cancer prevention look like in real life?
Understanding that prevention depends on access and environment raises an important question: If prevention isn’t just screening — and if it isn’t only about willpower — what does it actually look like in everyday life? Prevention becomes meaningful when it fits real lives, real schedules, and real environments.
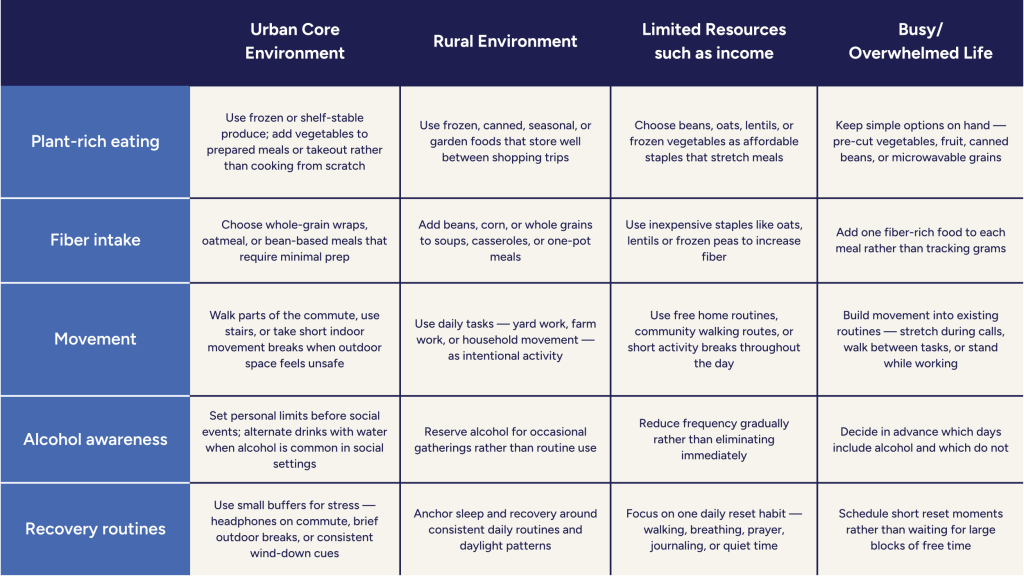
This is what prevention looks like in practice: not ideal routines, but adaptable patterns shaped within real circumstances.
From awareness to action
The question is no longer whether prevention matters but whether we are willing to invest in it. A recent analysis estimates that every dollar invested in building community exercise infrastructure, such as walking trails and parks, can return up to three dollars in direct health cost savings over time. For policymakers, this kind of return demonstrates how prevention infrastructure can strengthen both public health and fiscal responsibility.
That investment includes:
- integrating lifestyle conversations into routine care
- supporting community-based prevention programs
- improving access to nutritious food environments
- expanding opportunities for safe movement
- designing systems which focus on long-term health rather than reactive treatment
- When prevention is treated as infrastructure rather than advice, it becomes scalable.
The future of cancer prevention
The future of oncology will not be determined solely by better treatments. It will be defined by earlier action.
What might it look like if you brought that future a little closer next Monday morning? How can you take the first step—at home, in your clinic, or in your community—to move prevention from good intention to daily practice?
Lifestyle medicine is not an adjunct to cancer prevention. It is a foundation.
Risk reduction is not a single decision. It is a pattern built over time, supported by environments, and sustained by collective effort.
And the most powerful survivorship story remains the one that never has to begin.
Keep Learning. Take the Next Step.
LM for Cancer Risk Reduction and Survivorship Toolkit
Turn prevention into practice with a provider-focused, member-only toolkit featuring evidence summaries and ready-to-use patient handouts. This toolkit makes lifestyle medicine easier to implement in everyday clinical practice and daily life.
References
- Galicia Pacheco SI, Catena A, Sánchez MJ, et al. Socio-Economic Inequalities in Beliefs About Cancer and its Causes: Evidence From two Population Surveys. Psychooncology. 2024;33(12):e70035. doi:10.1002/pon.70035
- Schwartz LM, Woloshin S, Fowler FJ Jr, Welch HG. Enthusiasm for cancer screening in the United States. JAMA. 2004;291(1):71-78. doi:10.1001/jama.291.1.71
- Frank E, Tong E, Lobelo F, Carrera J, Duperly J. Physical activity levels and counseling practices of U.S. medical students. Med Sci Sports Exerc. 2008;40(3):413-421. doi:10.1249/MSS.0b013e31815ff399
- Kotseva K, De Bacquer D, De Backer G, et al. Lifestyle and risk factor management in people at high risk of cardiovascular disease. A report from the European Society of Cardiology European Action on Secondary and Primary Prevention by Intervention to Reduce Events (EUROASPIRE) IV cross-sectional survey in 14 European regions. Eur J Prev Cardiol. 2016;23(18):2007-2018. doi:10.1177/2047487316667784
- Braveman P, Gottlieb L. The social determinants of health: it’s time to consider the causes of the causes. Public Health Rep. 2014;129 Suppl 2(Suppl 2):19-31. doi:10.1177/00333549141291S206
- Henley SJ, Anderson RN, Thomas CC, Massetti GM, Peaker B, Richardson LC. Invasive Cancer Incidence, 2004-2013, and Deaths, 2006-2015, in Nonmetropolitan and Metropolitan Counties – United States. MMWR Surveill Summ. 2017;66(14):1-13. Published 2017 Jul 7. doi:10.15585/mmwr.ss6614a1
- Singh GK, Jemal A. Socioeconomic and Racial/Ethnic Disparities in Cancer Mortality, Incidence, and Survival in the United States, 1950-2014: Over Six Decades of Changing Patterns and Widening Inequalities. J Environ Public Health. 2017;2017:2819372. doi:10.1155/2017/2819372
- Islami F, Goding Sauer A, Miller KD, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J Clin. 2018;68(1):31-54. doi:10.3322/caac.21440
- World Cancer Research Fund/American Institute for Cancer Research. Diet, nutrition, physical activity and cancer: a global perspective. World Cancer Research Fund; 2018.
- American Institute for Cancer Research. Cancer prevention recommendations. https://www.aicr.org/cancer-prevention/
- Aune D, Chan DS, Lau R, et al. Dietary fibre, whole grains, and risk of colorectal cancer: systematic review and dose-response meta-analysis of prospective studies. BMJ. 2011;343:d6617. Published 2011 Nov 10. doi:10.1136/bmj.d6617
- McTiernan A, Friedenreich CM, Katzmarzyk PT, et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med Sci Sports Exerc. 2019;51(6):1252-1261. doi:10.1249/MSS.0000000000001937
- Rumgay H, Shield K, Charvat H, et al. Global burden of cancer in 2020 attributable to alcohol consumption: a population-based study. Lancet Oncol. 2021;22(8):1071-1080. doi:10.1016/S1470-2045(21)00279-5
- Lauby-Secretan B, Scoccianti C, Loomis D, et al. Body Fatness and Cancer–Viewpoint of the IARC Working Group. N Engl J Med. 2016;375(8):794-798. doi:10.1056/NEJMsr1606602
- American College of Lifestyle Medicine. Lifestyle medicine toolkit for cancer risk reduction and survivorship. https://lifestylemedicine.org. Accessed February 26, 2026.